Saturday, September 8, 2012
A little piece of history...
Quick update: Medonomics was silently shut down in July 2009 for fear that the statements made within may be too partisan/inflammatory and potentially viewed unfavorably by the many clients I have worked with over the years. My perspectives have, of course, evolved since these posts were written, and though I won't be contributing to this blog in the near future, I wanted to at least restore it and preserve a little piece of (my) history.
Monday, May 11, 2009
The Audacity of Citi & The Student Loan Corporation
By: Abhas Gupta
The email asks its recipients to support an online petition challenging the Obama administration's plan to directly administer student loans (through Direct Lending) and eliminate the middlemen (banks like Citigroup). The email provides several reasons to garner your support, but each of them is dishonest and intentionally misleading:
Direct Lending should improve our cost and ease of borrowing significantly. To quote the email, "This proposal impacts you as a citizen - both as a taxpayer and as a borrower", so please know the facts and don't get conned by your current provider. Here are two articles that describe the Direct Lending program and why Citi and others are putting up this ridiculous charade:
http://www.nytimes.com/2009/02/27/washington/27web-edu.html
http://www.nytimes.com/2009/04/13/us/politics/13student.html
Please share this with other medical students. It kills me that a few students may actually fall for this garbage and sign the petition.
References:
1. Thaler, Richard H. and Sunstein, Cass R. Nudge: Improving Decisions About Health, Wealth, and Happiness. 2008, Caravan Books
The email asks its recipients to support an online petition challenging the Obama administration's plan to directly administer student loans (through Direct Lending) and eliminate the middlemen (banks like Citigroup). The email provides several reasons to garner your support, but each of them is dishonest and intentionally misleading:
- "[Direct Lending] will eliminate your ability to choose a student loan provider" - to start, choice is not a factor when selecting student loans; instead, availability and the cost of borrowing are the factors students care about. As an aside, Sunstein and Thaler argue that the current system for choosing student loans is grossly inefficient1. Furthermore, nothing is stopping Citi from offering students loans after such legislation; Citi knows it simply can't be competitive without government guarantees and subsidies
- "[Direct Lending] will substantially increase the national debt" - amazing. Citi itself has taken $45b of US funds, made available by increasing the national debt. The top 10 student loan lenders have taken a total of $85b in bailout funds. I have no doubt that if all of the presently outstanding student loans were to default, they would not even come close to the $130b national debt courtesy of the financial industry
- "A variety of borrower benefits that lower your cost of borrowing" - I presume Citi is talking about direct-deposit discounts and such. Although I'm just speculating, I feel confident that Direct Lending will drop its interest rates to near the prime rate, so our cost of borrowing is going to be significantly better (tens of thousands of dollars cheaper) with Direct Lending than with private providers
- "Financial literacy programs that educate you on how to borrow responsibly" - the irony is staggering--Citi educating us on responsible borrowing. Much of the work of educating students is handled by financial aid departments, so I don't even know what value Citi adds for students
- "Web-based tools and resources to advise you about your financing options" - there are hundreds of free tools available online and with a single provider, I'm sure these free tools will become even more useful and easy to use
- "Default prevention services to help you pay back your loans" - these services are heavily subsidized by the government, not to mention that defaults are paid by the government, so we don't need to fear any negative change in our benefits. These subsidies will now to go towards providing other students with loans
Direct Lending should improve our cost and ease of borrowing significantly. To quote the email, "This proposal impacts you as a citizen - both as a taxpayer and as a borrower", so please know the facts and don't get conned by your current provider. Here are two articles that describe the Direct Lending program and why Citi and others are putting up this ridiculous charade:
http://www.nytimes.com/2009/02/27/washington/27web-edu.html
http://www.nytimes.com/2009/04/13/us/politics/13student.html
Please share this with other medical students. It kills me that a few students may actually fall for this garbage and sign the petition.
References:
1. Thaler, Richard H. and Sunstein, Cass R. Nudge: Improving Decisions About Health, Wealth, and Happiness. 2008, Caravan Books
Tuesday, April 1, 2008
Fleecing Medical Students: A Cost-Benefit Analysis of Step 2 CS
By: Abhas Gupta
As 4th-year rolls around, the inevitable costs of applying to residencies begin to weigh one down. The list seems endless: application fees, flights, lodging, new suit, new tie, PDA, and of course, licensing exams—Step 2 CS, alone, now costs $1050. Further investigation into the costs and benefits of Step 2 CS suggest that not all licensing requirements are constructive and perhaps, this time, medical students are being taken for a ride.
Why is Step 2 CS administered in the first place? The USMLE website states:
The cost of Step 2 CS to students is substantial; the $17.8 million calculated above does not even include the ancillary costs of traveling and housing—an additional $2 - $3 million—required to attend one of the only five nationwide testing centers. But what about the test's benefits, both to the student and to society? Presumably, identifying poor-performers is better for students and better for patients; students that need remediation are made aware of their weaknesses and patients are safer at the hands of well-vetted interns.
The relationship between Step 2 CS and these benefits is not as direct as suggested above. There are numerous mechanisms already in place to identify poor-performers both at the medical school and residency levels. A 1999 study published in Academic Medicine2 found that 48% of medical schools had incorporated standardized patients to evaluate the clinical skills of their students. One can reasonably expect that this fraction has increased since the study's publication. Also, all residency programs have numerous internal teaching tools and safety nets as well as external licensing requirements to cultivate and monitor their interns. The value of Step 2 CS can thus be considered minimal in the short term and all-but-useless by residency.
The justifications for an expensive Step 2 CS are therefore few and trivial. The following are three recommendations that could potentially mitigate the sizeable cost to students and still preserve the test's professional purpose:
With the excitement of the democratic primaries, I have been negligent in posting to this blog. If you have specific topics you would like to see discussed, please forward them here. I am currently considering writing on the health care payment system and pay-for-performance incentives.
References:
1. 2006 USMLE Performance Data.
2. Kassebaum, DG, Eaglen, RH. Shortcomings in the Evaluation of Students’ Clinical Skills and Behaviors in Medical School
As 4th-year rolls around, the inevitable costs of applying to residencies begin to weigh one down. The list seems endless: application fees, flights, lodging, new suit, new tie, PDA, and of course, licensing exams—Step 2 CS, alone, now costs $1050. Further investigation into the costs and benefits of Step 2 CS suggest that not all licensing requirements are constructive and perhaps, this time, medical students are being taken for a ride.
Why is Step 2 CS administered in the first place? The USMLE website states:
Step 2 CS uses standardized patients to test medical students and graduates on their ability to gather information from patients, perform physical examinations, and communicate their findings to patients and colleagues.The NBME® reports that in the 2005 academic year, 16,936 medical students took the Step 2 CS and 98% passed2. Of the test takers, 325 had failed previously but overwhelmingly passed this time around (97%) . Put another way: In the 2005 academic year, 4th-year medical students were made to spend $17.8 million (16,936 students x $1050/student) on Step 2 CS alone so that 363 students with unsatisfactory clinical skills could be identified and retested. After retesting, only about 11 students would still fall short of satisfactory clinical proficiency.
The cost of Step 2 CS to students is substantial; the $17.8 million calculated above does not even include the ancillary costs of traveling and housing—an additional $2 - $3 million—required to attend one of the only five nationwide testing centers. But what about the test's benefits, both to the student and to society? Presumably, identifying poor-performers is better for students and better for patients; students that need remediation are made aware of their weaknesses and patients are safer at the hands of well-vetted interns.
The relationship between Step 2 CS and these benefits is not as direct as suggested above. There are numerous mechanisms already in place to identify poor-performers both at the medical school and residency levels. A 1999 study published in Academic Medicine2 found that 48% of medical schools had incorporated standardized patients to evaluate the clinical skills of their students. One can reasonably expect that this fraction has increased since the study's publication. Also, all residency programs have numerous internal teaching tools and safety nets as well as external licensing requirements to cultivate and monitor their interns. The value of Step 2 CS can thus be considered minimal in the short term and all-but-useless by residency.
The justifications for an expensive Step 2 CS are therefore few and trivial. The following are three recommendations that could potentially mitigate the sizeable cost to students and still preserve the test's professional purpose:
- Implement other metrics to identify students at high-risk for failing the Step 2 CS - factors such as scores on Step 1 or Step 2 CK, serious clinical infractions, or consistently poor-performance in clerkships could help identify students with clinical skills weaknesses. The Step 2 CS could then be made mandatory for these students and these students only
- Minimize redundancy in clinical skills testing – many institutions already test clinical skills, albeit with different formats and styles. The NBME could establish a set of national guidelines dictating how the evaluation should be conducted. Students at institutions that comply with these guidelines would then be exempt from taking the Step 2 CS
- Eliminate Step 2 CS from residency programs' entrance criteria – leadership from these programs is necessary for students and medical school administrators to consider any changes to the current system. These programs should be made aware of the negligible benefit of Step 2 CS and come to the aid of their future interns
With the excitement of the democratic primaries, I have been negligent in posting to this blog. If you have specific topics you would like to see discussed, please forward them here. I am currently considering writing on the health care payment system and pay-for-performance incentives.
References:
1. 2006 USMLE Performance Data.
2. Kassebaum, DG, Eaglen, RH. Shortcomings in the Evaluation of Students’ Clinical Skills and Behaviors in Medical School
Monday, January 14, 2008
Dissecting the Democratic Front-Runners' Health Care Plans
By: Abhas Gupta
Cost-Containment
Although cost is an important component of any policy, I do not believe it is as important here as the candidates' measures to control cost growth*. The candidates' plans are very similar†. They both support prevention and chronic care initiatives. They support the government's right to negotiate drug prices and they want to level the payment gap between Medicare Advantage and traditional Medicare. They both support legislation to limit insurance companies' latitude in denying coverage to individuals. They both wish to create a national health insurance pool that is overseen by the public, similar to the Federal Employee Health Benefits Plan. Despite these commonalities, the candidates' plan do differ on several important points:
Coverage
"47 million Americans do not have..." - I'm sure you've heard the stump speech. The candidates have squabbled about whose plan covers more Americans, acknowledging, though, that they both are aspiring to a truly universal health care system. Mandates often come up in the discussion of coverage--Clinton supports a mandate that all Americans purchase coverage and Obama supports a mandate only for children--but there are broad, false perceptions that the lack of a mandate implies an aversion to universal coverage. Before we get into the specifics, let's take a look at the make-up of the 47 million uninsured:
Like I said before, both candidates' plans are very similar, yet I am inclined to more strongly support Senator Obama's plan. I firmly believe that greater private competition in a public-defined playing field is what's needed to improve our health care system--the Obama plan's National Health Insurance Exchange most closely captures this sentiment. I also strongly oppose a mandate as a matter of principle, but more importantly, because we are likely facing a recession and a mandate would only serve to exacerbate our economic troubles.
* I expect that both plans will probably cost within $50 billion of each other. This is rather insignificant when we are spending $2 trillion on health care and our costs are growing at 7%+ annually
† Obama released his plan in May 2007 and Clinton released her plan in August 2007
‡ I suspect that Obama led the effort behind the NEJM article. The thesis of the article--making patients the centerpiece of any reforms and framing physician and litigators positions around patients--has Obama's signature all over it
§ Real economists unlike Krugman, who's at it again: in the same article, he mentions both Obama's and Hillary's economic stimulus packages and hints at their health care plans, yet he conveniently does not mention impact of a mandate on economic growth
References:
1. Health08.org, 2008 Presidential Candidates Health Care Proposals: Side-by-Side Summary. The Kaiser Family Foundation. September 5, 2007
2. Health Care Spending and the Uninsured. Douglas Holtz-Eakin. Congressional Budget Office, January 28, 2004
3. Plan for a Healthy America. Obama for America. http://www.barackobama.com/issues/healthcare/
4. American Health Choices Plan. Hillary Clinton for President. http://www.hillaryclinton.com/feature/healthcareplan/
Cost-Containment
Although cost is an important component of any policy, I do not believe it is as important here as the candidates' measures to control cost growth*. The candidates' plans are very similar†. They both support prevention and chronic care initiatives. They support the government's right to negotiate drug prices and they want to level the payment gap between Medicare Advantage and traditional Medicare. They both support legislation to limit insurance companies' latitude in denying coverage to individuals. They both wish to create a national health insurance pool that is overseen by the public, similar to the Federal Employee Health Benefits Plan. Despite these commonalities, the candidates' plan do differ on several important points:
- Insurance Industry Regulation - Obama supports the formation of a 'National Health Insurance Exchange', which is hands-down the biggest difference between the candidates' cost-cutting plans. Obama wants this central group to establish coverage criteria, even going so far as to set a minimum on the portion of premiums that must be paid out in benefits. The elements of disclosing cost and value to consumers is hinted at by Clinton's "Best Practices Institute" (discussed below), but the extent of insurance regulation is far more aggressive in the Obama plan. His plan could quickly cut tens of billions out of cost while simultaneously drawing attention to the gaps and inconsistencies in private insurance plans
- Health Care Quality and Value - Clinton supports a "Best Practices Institute" with the goal of helping consumers make the "right care choices." Obama explicitly requires that hospitals and providers need to publicly report measures of cost and quality. I expect both proposals have the same end goal, but Clinton wants this to be a government-run effort whereas Obama enables outside groups to take on the task
- Malpractice Reform - I previously commented on Clinton and Obama's joint letter to NEJM on making patient rights the centerpiece of malpractice reform. Clinton's plan only mentions additional physician protections, whereas Obama endorses "new models", presumably the ones they jointly outlined in the NEJM article and MEDiC bill. I previously expressed my strong support for systems-based approaches to malpractice reform. I am at a loss for why Clinton left this out of her plan‡
- Drug Prices - Both plans want to promote generic drug use. Clinton explicitly wishes to alter patent protections to favor generic drugs. Additionally, Clinton wishes to limit (but not eliminate?) direct-to-consumer advertising, an impressive undertaking, but I'm skeptical about its legality and prospects on the floor. Obama supports the reimportation of drugs, another laudable undertaking, but I am again skeptical of its prospects
- Electronic Medical Records - Both support a "paperless system", but Obama calls for an immediate $50 billion investment ($10 billion over 5 years) towards EMR adoption
Coverage
"47 million Americans do not have..." - I'm sure you've heard the stump speech. The candidates have squabbled about whose plan covers more Americans, acknowledging, though, that they both are aspiring to a truly universal health care system. Mandates often come up in the discussion of coverage--Clinton supports a mandate that all Americans purchase coverage and Obama supports a mandate only for children--but there are broad, false perceptions that the lack of a mandate implies an aversion to universal coverage. Before we get into the specifics, let's take a look at the make-up of the 47 million uninsured:
- Duration: 45% of the uninsured remain so for less than four months
- Age-distribution: 25% are under 18 and 14% are under 25
- Income: 75% are under twice the poverty line
- Employment: 46% are part-time employees, 10% are unemployed
- Employer: 59% are employed at small businesses of less than 100 employees
- Health: 86% consider themselves in good to excellent health
- Children and Young Adults (Under 25, 39% of the uninsured) - Both plans expand SCHIP to cover all children under 18, but differ in their approach to the 18 to 25-year-olds. Obama's plan is relatively simple in this regard: He enables this group to be covered under their families' plans and he expands SCHIP to cover those still uninsured. Clinton applies her health care mandate to 18-25 year olds, so these adults would have to purchase individual health insurance. Although these individuals utilize only a few billion dollars of health care annually, they will be asked to pay out tens of billions under the Clinton plan. I find this position difficult to justify, but I suppose one can argue that the development of chronic illnesses is shaped by factors early in life and thus all ages should bear an equal share of the health care pie
- Small Business Employees (59% of the uninsured) - Both Clinton and Obama allow small businesses to pool their risk by buying into a national, public-moderated plan. Clinton mandates all small businesses to purchase health insurance, except if it has less than 25 employees. She offers tax credits to help offset these purchasing costs. Employees of small businesses with less than 25 employees would have to purchase individual insurance and would also be given tax credits to help shoulder the cost. Obama offers similar tax incentives to small businesses, but does not institute a mandate. I believe this decision is rooted in Obama's philosophy that businesses and individuals would buy health insurance if it was affordable. Assuming this is true, I suspect Obama wants to show businesses that his cost-cutting policies can slow the growth of health care costs or even reduce them. Businesses could then budget and purchase health insurance without fear of exploding benefits costs. Small businesses would then buy health care to attract competitive employees and the issue of a mandate would be subsequently moot
- Poor Americans (75% of the uninsured) - both candidates will raise Medicaid's eligibility requirements, but neither offers any details on how many individuals will be covered. A Clinton mandate would require those who are ineligible for Medicaid (because they make slightly above the minimum income) to purchase health insurance
Like I said before, both candidates' plans are very similar, yet I am inclined to more strongly support Senator Obama's plan. I firmly believe that greater private competition in a public-defined playing field is what's needed to improve our health care system--the Obama plan's National Health Insurance Exchange most closely captures this sentiment. I also strongly oppose a mandate as a matter of principle, but more importantly, because we are likely facing a recession and a mandate would only serve to exacerbate our economic troubles.
* I expect that both plans will probably cost within $50 billion of each other. This is rather insignificant when we are spending $2 trillion on health care and our costs are growing at 7%+ annually
† Obama released his plan in May 2007 and Clinton released her plan in August 2007
‡ I suspect that Obama led the effort behind the NEJM article. The thesis of the article--making patients the centerpiece of any reforms and framing physician and litigators positions around patients--has Obama's signature all over it
§ Real economists unlike Krugman, who's at it again: in the same article, he mentions both Obama's and Hillary's economic stimulus packages and hints at their health care plans, yet he conveniently does not mention impact of a mandate on economic growth
References:
1. Health08.org, 2008 Presidential Candidates Health Care Proposals: Side-by-Side Summary. The Kaiser Family Foundation. September 5, 2007
2. Health Care Spending and the Uninsured. Douglas Holtz-Eakin. Congressional Budget Office, January 28, 2004
3. Plan for a Healthy America. Obama for America. http://www.barackobama.com/issues/healthcare/
4. American Health Choices Plan. Hillary Clinton for President. http://www.hillaryclinton.com/feature/healthcareplan/
Friday, November 23, 2007
Medical Malpractice and Tort Reform: A Brief Overview and Case Study
By: Abhas Gupta
Empirical Research on Medical Malpractice
Several studies were conducted over the past three decades to better understand medical malpractice litigation. Two studies (NEJM 1977; NEJM 1990) looked at the medical records of thousands of patients in California and New York, respectively. Both found similar rates of iatrogenic injury (~4%). Of these cases, only a fraction were due to negligence (about a quarter, or 1% overall) and an even smaller fraction of those cases actually resulted in malpractice claims. Another study (NEJM 1996) found that compensation in medical malpractice cases was, erroneously, more often proportional to the plaintiff’s degree of disability than the defendant’s degree of negligence.
A recent retrospective study (NEJM 2006) inspected 1452 closed malpractice claims from five insurers. The study found that 3% of claims had no injury and 37% had no errors; therefore, 40% of the claims were found to be frivolous. Fortunately, most frivolous claims (>70%) did not result in payment, but of course, the cost of defending against these claims was ultimately bore out by the defendants. Of the claims deemed valid by the authors, 73% resulted in payment. The most shocking finding of the study was that 54 cents of every $1 in compensation did not go to patients; instead, the bulk of payouts were absorbed by trial attorneys and legal fees.
There is currently little evidence relating litigation with subsequent rates of adverse events, negligence rates, or quality-of-care indicators. This questions the ideology of malpractice litigation as a means of deterring unsafe practices. Moreover, there are a number of studies showing that litigation influences physician behavior in undesirable ways (by promoting defensive medicine, for example). Nevertheless, there is a glaring theme connecting all of these studies: our system of distributing compensation for victims of negligence is insufficient and profoundly inefficient.
Tort Reform: Punitive vs. Systems-based Approaches
 Tort reform proponents can be crudely divided into two schools of thought: the first seeks to limit the threat of litigation (conventional tort reform) and the second pursues non-punitive, systems-oriented approaches to limit both errors and court cases (system reform). Patient safety groups largely occupy the second school of thought. They advocate systems-based approaches, implying that physicians are not the only ones to blame for medical errors--our hospital and health care systems are also responsible. The table4 on the right categorizes many of the current approaches being considered/implemented in tort reform.
Tort reform proponents can be crudely divided into two schools of thought: the first seeks to limit the threat of litigation (conventional tort reform) and the second pursues non-punitive, systems-oriented approaches to limit both errors and court cases (system reform). Patient safety groups largely occupy the second school of thought. They advocate systems-based approaches, implying that physicians are not the only ones to blame for medical errors--our hospital and health care systems are also responsible. The table4 on the right categorizes many of the current approaches being considered/implemented in tort reform.
A Long-term Strategy for Controlling Malpractice Costs
As physicians, we need to agree that patients are at the heart of any reform and we should frame our positions as such. We must vehemently advocate, on behalf our patients, that 1) victims of negligence should be compensated quickly and appropriately; and 2) medical errors should be acknowledged and investigated in order for adequate solutions to be implemented. Given the concordance of these values with those of patient-safety groups, our camps should join forces and embrace the push for non-punitive, systems-oriented approaches (described above).
The costs of acknowledging our mistakes will surely be large in the short-term. Arguably, these costs could be on par with current malpractice costs because the corresponding increase in claims would be offset by the decrease in payout amounts (made possible by side-stepping trial attorneys and their substantial fees). Over time, we can expect the incidence of medical errors to decrease--through recognition and corrective action--thereby reducing malpractice costs over the long-term.
Case Study: The University of Michigan Health System
In 2002, the University of Michigan Health System launched their Medical Error Disclosure program with the following three principles: The hospital system has only made public three findings from this program (see figure on right). Over the course of four years, a substantial decrease occurred in annual litigation costs, average time to resolution of claims, and the total number of claims. Although not reported, the overall cost of malpractice claims* can be expected to decrease as well.
The hospital system has only made public three findings from this program (see figure on right). Over the course of four years, a substantial decrease occurred in annual litigation costs, average time to resolution of claims, and the total number of claims. Although not reported, the overall cost of malpractice claims* can be expected to decrease as well.
In 2006, Senators Obama and Clinton co-sponsored the National Medical Error Disclosure and Compensation (MEDiC) bill3 that created funding for hospitals to undertake programs similar to UMHS. The bill affords legal protections to hospitals who disclose errors voluntarily to the patient. Also, the bill includes an important stipulation that a percent of the savings in malpractice costs, attained by implementing the strategies outlined in MEDiC, would then have to be applied to improve patient safety and further reduce medical errors. The bill also called for the creation of an Office of Patient Safety and Health Care Quality which would assess patient safety issues nationwide and serve as the primary vehicle for disseminating best practices throughout the health care system.
*Adjusted for fluctuations in staff, regional malpractice rates, etc. and notwithstanding the underwriting structure (individual physicians vs. hospital systems)
Note: If you are interested in learning more, begin by reading Medical Malpractice (NEJM 2004). This post summarizes a lot of the concepts that are presented with greater detail by Studdert et al.
References:
1. California Medical Association and California Hospital Association report on the Medical Insurance Feasibility Study. Mills DH, ed. San Francisco, CA: 1977
2. Claims, Errors, and Compensation Payments in Medical Malpractice Litigation. DM Studdert, MM Mello, AA Gawande, TK Gandhi, A …. NEJM, 2006
3. Making Patient Safety the Centerpiece of Medical Liability Reform. HR Clinton, B Obama. NEJM, 2006
4. Medical Malpractice. DM Studdert, MM Mello, TA Brennan. NEJM, 2004
5. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York: report of the Harvard Medical Practice Study to the state of New York. Harvard Medical Practice Study. Cambridge, MA: 1990
6. Relation between Negligent Adverse Events and the Outcomes of Medical-Malpractice Litigation. TA Brennan, CM Sox, HR Burstin. NEJM, 1996
Empirical Research on Medical Malpractice
Several studies were conducted over the past three decades to better understand medical malpractice litigation. Two studies (NEJM 1977; NEJM 1990) looked at the medical records of thousands of patients in California and New York, respectively. Both found similar rates of iatrogenic injury (~4%). Of these cases, only a fraction were due to negligence (about a quarter, or 1% overall) and an even smaller fraction of those cases actually resulted in malpractice claims. Another study (NEJM 1996) found that compensation in medical malpractice cases was, erroneously, more often proportional to the plaintiff’s degree of disability than the defendant’s degree of negligence.
A recent retrospective study (NEJM 2006) inspected 1452 closed malpractice claims from five insurers. The study found that 3% of claims had no injury and 37% had no errors; therefore, 40% of the claims were found to be frivolous. Fortunately, most frivolous claims (>70%) did not result in payment, but of course, the cost of defending against these claims was ultimately bore out by the defendants. Of the claims deemed valid by the authors, 73% resulted in payment. The most shocking finding of the study was that 54 cents of every $1 in compensation did not go to patients; instead, the bulk of payouts were absorbed by trial attorneys and legal fees.
There is currently little evidence relating litigation with subsequent rates of adverse events, negligence rates, or quality-of-care indicators. This questions the ideology of malpractice litigation as a means of deterring unsafe practices. Moreover, there are a number of studies showing that litigation influences physician behavior in undesirable ways (by promoting defensive medicine, for example). Nevertheless, there is a glaring theme connecting all of these studies: our system of distributing compensation for victims of negligence is insufficient and profoundly inefficient.
Tort Reform: Punitive vs. Systems-based Approaches
 Tort reform proponents can be crudely divided into two schools of thought: the first seeks to limit the threat of litigation (conventional tort reform) and the second pursues non-punitive, systems-oriented approaches to limit both errors and court cases (system reform). Patient safety groups largely occupy the second school of thought. They advocate systems-based approaches, implying that physicians are not the only ones to blame for medical errors--our hospital and health care systems are also responsible. The table4 on the right categorizes many of the current approaches being considered/implemented in tort reform.
Tort reform proponents can be crudely divided into two schools of thought: the first seeks to limit the threat of litigation (conventional tort reform) and the second pursues non-punitive, systems-oriented approaches to limit both errors and court cases (system reform). Patient safety groups largely occupy the second school of thought. They advocate systems-based approaches, implying that physicians are not the only ones to blame for medical errors--our hospital and health care systems are also responsible. The table4 on the right categorizes many of the current approaches being considered/implemented in tort reform.A Long-term Strategy for Controlling Malpractice Costs
As physicians, we need to agree that patients are at the heart of any reform and we should frame our positions as such. We must vehemently advocate, on behalf our patients, that 1) victims of negligence should be compensated quickly and appropriately; and 2) medical errors should be acknowledged and investigated in order for adequate solutions to be implemented. Given the concordance of these values with those of patient-safety groups, our camps should join forces and embrace the push for non-punitive, systems-oriented approaches (described above).
The costs of acknowledging our mistakes will surely be large in the short-term. Arguably, these costs could be on par with current malpractice costs because the corresponding increase in claims would be offset by the decrease in payout amounts (made possible by side-stepping trial attorneys and their substantial fees). Over time, we can expect the incidence of medical errors to decrease--through recognition and corrective action--thereby reducing malpractice costs over the long-term.
Case Study: The University of Michigan Health System
In 2002, the University of Michigan Health System launched their Medical Error Disclosure program with the following three principles:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly
- Aggressively defend cases that the hospital considers to be without merit
- Study all adverse events to determine improvements
 The hospital system has only made public three findings from this program (see figure on right). Over the course of four years, a substantial decrease occurred in annual litigation costs, average time to resolution of claims, and the total number of claims. Although not reported, the overall cost of malpractice claims* can be expected to decrease as well.
The hospital system has only made public three findings from this program (see figure on right). Over the course of four years, a substantial decrease occurred in annual litigation costs, average time to resolution of claims, and the total number of claims. Although not reported, the overall cost of malpractice claims* can be expected to decrease as well. In 2006, Senators Obama and Clinton co-sponsored the National Medical Error Disclosure and Compensation (MEDiC) bill3 that created funding for hospitals to undertake programs similar to UMHS. The bill affords legal protections to hospitals who disclose errors voluntarily to the patient. Also, the bill includes an important stipulation that a percent of the savings in malpractice costs, attained by implementing the strategies outlined in MEDiC, would then have to be applied to improve patient safety and further reduce medical errors. The bill also called for the creation of an Office of Patient Safety and Health Care Quality which would assess patient safety issues nationwide and serve as the primary vehicle for disseminating best practices throughout the health care system.
*Adjusted for fluctuations in staff, regional malpractice rates, etc. and notwithstanding the underwriting structure (individual physicians vs. hospital systems)
Note: If you are interested in learning more, begin by reading Medical Malpractice (NEJM 2004). This post summarizes a lot of the concepts that are presented with greater detail by Studdert et al.
References:
1. California Medical Association and California Hospital Association report on the Medical Insurance Feasibility Study. Mills DH, ed. San Francisco, CA: 1977
2. Claims, Errors, and Compensation Payments in Medical Malpractice Litigation. DM Studdert, MM Mello, AA Gawande, TK Gandhi, A …. NEJM, 2006
3. Making Patient Safety the Centerpiece of Medical Liability Reform. HR Clinton, B Obama. NEJM, 2006
4. Medical Malpractice. DM Studdert, MM Mello, TA Brennan. NEJM, 2004
5. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York: report of the Harvard Medical Practice Study to the state of New York. Harvard Medical Practice Study. Cambridge, MA: 1990
6. Relation between Negligent Adverse Events and the Outcomes of Medical-Malpractice Litigation. TA Brennan, CM Sox, HR Burstin. NEJM, 1996
Medical Malpractice: A State of Crisis
By: Abhas Gupta

Besides carving into hospital and physician profits, high malpractice insurance rates may also eventually threaten patient care by driving physicians out of high premium areas. Some have reported that the impact on patients' access to care is modest1 and others have reported an increase in physician influx to states following the introduction of malpractice caps. Irrespective of this debate, the impact on physician profits and morale is substantial.
The General Accounting Office (GAO) undertook a study2 in 2003 to investigate why malpractice rates were increasing so rapidly. They cited a number of reasons, some of which are not immediately obvious:
References:
1. Changes in Physician Supply and Scope of Practice During a Malpractice Crisis: Evidence from Pennsylvania. M Mello et al. Health Affairs, 2007
2. GAO-03-702 Medical Malpractice Insurance: Multiple Factors Have Contributed to Increased Premium Rates. General Accounting Office, June 2003
3. Current Award Trends in Personal Injury. 43rd ed. Jury Verdict Research. Horsham, PA.

Besides carving into hospital and physician profits, high malpractice insurance rates may also eventually threaten patient care by driving physicians out of high premium areas. Some have reported that the impact on patients' access to care is modest1 and others have reported an increase in physician influx to states following the introduction of malpractice caps. Irrespective of this debate, the impact on physician profits and morale is substantial.
The General Accounting Office (GAO) undertook a study2 in 2003 to investigate why malpractice rates were increasing so rapidly. They cited a number of reasons, some of which are not immediately obvious:
- Previously underpriced premiums - In the '90s, underwriters/insurers initially kept malpractice premiums high in anticipation of another malpractice crisis. However, the reality was less bleak: the number of claims stabilized and the financial markets were performing well. The result was an opportunity for other insurers to step in and undercut competitors. This practice became so intense that many insurers eventually underpriced their premiums to increase their subscriber base. All this was feasible, however, until the number of claims started increasing and the market trajectory changed course
- Downturn in the economy – as the economy slowed, insurers' investment returns suffered and the difference (between projections and actual growth) had to be bridged by increasing premiums
 Increases in claims and payouts - beginning in 1999, the median size of payouts increased precipitously (see the figure3 on the right). The GAO offers up a number of factors that may have contributed to this increase, including greater public awareness of medical errors (To Err Is Human was published around this time), lower levels of confidence and trust in the health care system (possibly due to managed care), improvements in diagnostic technology that in turn increased the intensity of care, rising public expectations about medical care, and an increasing reluctance of plaintiffs to accept settlements.
Increases in claims and payouts - beginning in 1999, the median size of payouts increased precipitously (see the figure3 on the right). The GAO offers up a number of factors that may have contributed to this increase, including greater public awareness of medical errors (To Err Is Human was published around this time), lower levels of confidence and trust in the health care system (possibly due to managed care), improvements in diagnostic technology that in turn increased the intensity of care, rising public expectations about medical care, and an increasing reluctance of plaintiffs to accept settlements.

References:
1. Changes in Physician Supply and Scope of Practice During a Malpractice Crisis: Evidence from Pennsylvania. M Mello et al. Health Affairs, 2007
2. GAO-03-702 Medical Malpractice Insurance: Multiple Factors Have Contributed to Increased Premium Rates. General Accounting Office, June 2003
3. Current Award Trends in Personal Injury. 43rd ed. Jury Verdict Research. Horsham, PA.
Tuesday, November 6, 2007
The Most Efficient Walking Path Between Two Points on the Manhattan Grid
By: Abhas Gupta
Like many New Yorkers, I think about the same question every time I get out of the subway: What is the fastest way to get to where I'm going? And every time, I simply walk in the general direction of my destination, letting traffic lights dictate my specific path. I asked my better half about her method to getting places quickly and she replied, "It's easy! Just time the lights." Although this may be good advice for the seasoned New Yorker traveling at the speed of traffic, I suggest the following, more generalizable approach.
First, let's break the problem down into three simple cases:
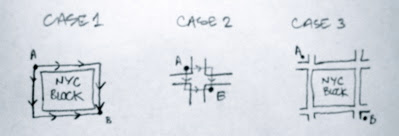
Case 1 - the two possible paths here are of the same distance and have no additional variables (traffic lights, stop signs, etc.); therefore, both paths are equivalent.
Case 2 - the two possible paths here involve crossing one street and one avenue. The order is determined by which direction has the green light first.
Case 3 - here, all of the possible paths have the same distance and the same number of "obstacles" (two avenues and two streets to cross). This example can be easily extended to more complicated cases. In fact, all paths on an ideal grid--one where all streets are parallel, all avenues are parallel, and all streets are perpendicular to all avenues--have the same distance. Coincidentally, this distance is called the Manhattan distance. So how does one determine the most efficient path?
First, we need to identify the inherent differences between crossing a typical street and a typical avenue in Manhattan. Streets frequently have less traffic and fewer lanes. Streets can also be easily crossed when a light is red. Avenues, on the other hand, typically have more traffic and more lanes, making it difficult to cross unless the light is green. Finally, lights for avenues remain green for a longer period of time, so multiple streets can be traversed without stopping at a light, whereas the same is not the case for multiple avenues.
The fastest path between any two points obviously avoids getting stuck at a light. The solution then boils down to which path has a lower probability of getting stuck at a light. Since streets are easier to cross than avenues, the fastest path would lend priority to crossing avenues (since they are more difficult to cross). Also, depending on the distance that needs to be traveled, waiting a few seconds at an intersection in order to cross an avenue could be advantageous over proceeding to the next intersection. To summarize, the most efficient walking path can be achieved by following these simple rules:
Like many New Yorkers, I think about the same question every time I get out of the subway: What is the fastest way to get to where I'm going? And every time, I simply walk in the general direction of my destination, letting traffic lights dictate my specific path. I asked my better half about her method to getting places quickly and she replied, "It's easy! Just time the lights." Although this may be good advice for the seasoned New Yorker traveling at the speed of traffic, I suggest the following, more generalizable approach.
First, let's break the problem down into three simple cases:

Case 1 - the two possible paths here are of the same distance and have no additional variables (traffic lights, stop signs, etc.); therefore, both paths are equivalent.
Case 2 - the two possible paths here involve crossing one street and one avenue. The order is determined by which direction has the green light first.
Case 3 - here, all of the possible paths have the same distance and the same number of "obstacles" (two avenues and two streets to cross). This example can be easily extended to more complicated cases. In fact, all paths on an ideal grid--one where all streets are parallel, all avenues are parallel, and all streets are perpendicular to all avenues--have the same distance. Coincidentally, this distance is called the Manhattan distance. So how does one determine the most efficient path?
First, we need to identify the inherent differences between crossing a typical street and a typical avenue in Manhattan. Streets frequently have less traffic and fewer lanes. Streets can also be easily crossed when a light is red. Avenues, on the other hand, typically have more traffic and more lanes, making it difficult to cross unless the light is green. Finally, lights for avenues remain green for a longer period of time, so multiple streets can be traversed without stopping at a light, whereas the same is not the case for multiple avenues.
The fastest path between any two points obviously avoids getting stuck at a light. The solution then boils down to which path has a lower probability of getting stuck at a light. Since streets are easier to cross than avenues, the fastest path would lend priority to crossing avenues (since they are more difficult to cross). Also, depending on the distance that needs to be traveled, waiting a few seconds at an intersection in order to cross an avenue could be advantageous over proceeding to the next intersection. To summarize, the most efficient walking path can be achieved by following these simple rules:
- When given an equal choice of direction (like Case 1), travel towards the next avenue (thereby maximizing opportunities to cross avenues)
- When the path requires crossing multiple avenues, consider waiting at an intersection to cross the avenue instead of proceeding to the next intersection
- Treat crosstown streets like avenues (since they have the same risk of getting stuck at a light)
Subscribe to:
Posts (Atom)
 ABHAS GUPTA
ABHAS GUPTA